How to perform a lateral neck approach for penetrating neck trauma
Source
To access the full video and additional content on this subject, log in or subscribe
Summary
Focus: Lateral neck approach for exposing critical vascular structures of the neck for diagnosis and treatment.
Key elements: Patient positioning, incision planning, carotid sheath exposure, carotid and internal jugular vein control, access to medial structures, hemostasis, closure, pitfalls, complications, and aftercare.
Indications and Clinical Context
General
Medical experts: Ville Vänni, trauma surgeon
Name of procedure: Lateral neck approach for penetrating neck trauma
Goal of Operation
To expose critical vascular structures of the neck for diagnosis and treatment.
Problem
Penetrating neck injury: vascular injury, tracheal injury, esophageal injury, cranial nerve injuries.
Diagnosis
Open wound of neck (ICD-10: S11.0–S11.9)
Larynx and trachea (S11.0)
Thyroid gland (S11.1)
Pharynx and cervical esophagus (S11.2)
Other specified parts of neck (S11.8)
Unspecified part of neck (S11.9)
Injury of blood vessels at neck level (ICD-10: S15.0–S15.9)
Carotid artery (S15.0)
Vertebral artery (S15.1)
External jugular vein (S15.2)
Internal jugular vein (S15.3)
Other specified blood vessels (S15.8)
Unspecified blood vessels (S15.9)
Short Pathophysiological Description
Penetrating neck injuries breach the platysma muscle and potentially damage vital structures within the confined cervical space, including major vascular structures, airway, upper gastrointestinal tract, and cranial nerves. The injury creates direct tissue trauma through laceration or transection of anatomical structures, while projectiles, such as bullets, fragments, or other high-velocity objects, may cause additional cavitation effects that extend damage beyond the immediate wound tract.
Vascular injury leads to hemorrhage that can compromise airway patency through external compression or hematoma formation, while damage to the trachea or esophagus creates immediate life-threatening complications. The proximity of critical structures means that even small penetrating wounds can cause multiple organ system injuries, with the potential for rapid decompensation due to airway obstruction, exsanguination, or aspiration from combined aerodigestive tract injuries.
Key Anatomical Structures
Common carotid artery
Carotid bifurcation
Internal carotid artery
Carotid sinus
External carotid artery
Superior thyroid artery
Other branches
Internal jugular vein
Facial vein
Larynx
Trachea
Esophagus
Thyroid gland
Vagus nerve
Recurrent laryngeal nerve
Superior laryngeal nerve
Hypoglossal nerve (CN XII)
Glossopharyngeal nerve (CN IX)
Ansa cervicalis
Platysma
Sternocleidomastoid muscle
Omohyoid muscle
Strap muscles
Digastric muscle
Step-by-Step Technique
Patient Positioning, Anesthesia, and Preparation
The patient is positioned supine under general anesthesia with endotracheal intubation secured.
A small bump is placed under the shoulders to extend the neck, improving surgical access.
The head is rotated toward the contralateral side of the incision, exposing the sternocleidomastoid muscle and lateral neck structures.
Intravenous access is established on the side opposite to the surgical site.
Sterile preparation and draping extend to include the chest and clavicles, allowing for potential proximal extension of the incision if control of proximal vascular structures becomes necessary.
Procedural Goals and Approach Strategy
The lateral neck approach provides systematic access to the major vascular structures, neural structures, and upper aerodigestive tract following penetrating neck trauma. Structures can be systematically evaluated for injury and either repaired or documented for subsequent management. If needed, the approach can be performed unilaterally, bilaterally, or combined with a collar incision or sternotomy, depending on the extent and location of the injury.
The critical vascular structures that may be injured and require exploration are the common carotid, internal and external carotid arteries, and the internal jugular vein, with exposure allowing for assessment and determination of appropriate treatment while preserving adjacent neural structures.
Critical neural structures that must be preserved include the vagus nerve within the carotid sheath, the hypoglossal nerve crossing near the carotid bifurcation, the glossopharyngeal nerve in the upper neck, and the recurrent laryngeal nerve running between the trachea and esophagus.
The neck is classically divided into three anatomical zones for surgical planning. While modern trauma management has largely moved beyond zone-based decision making, these zones remain useful for describing injury location and understanding access limitations.
Zone 1 extends from the clavicles to the cricoid cartilage and contains the great vessels arising from the brachiocephalic trunk. Injuries here may require median sternotomy for adequate proximal vascular control.
Zone 2 extends from the cricoid cartilage to the angle of the mandible and contains the major cervical vascular structures and upper aerodigestive tract. Zone 2 is most accessible through the lateral approach.
Zone 3 extends from the angle of the mandible to the skull base. Here, surgical access is limited by restricted operative space and risk to cranial nerves, making endovascular repair the preferred treatment for vascular injuries.
Log in or subscribe to access full content and see all the images.
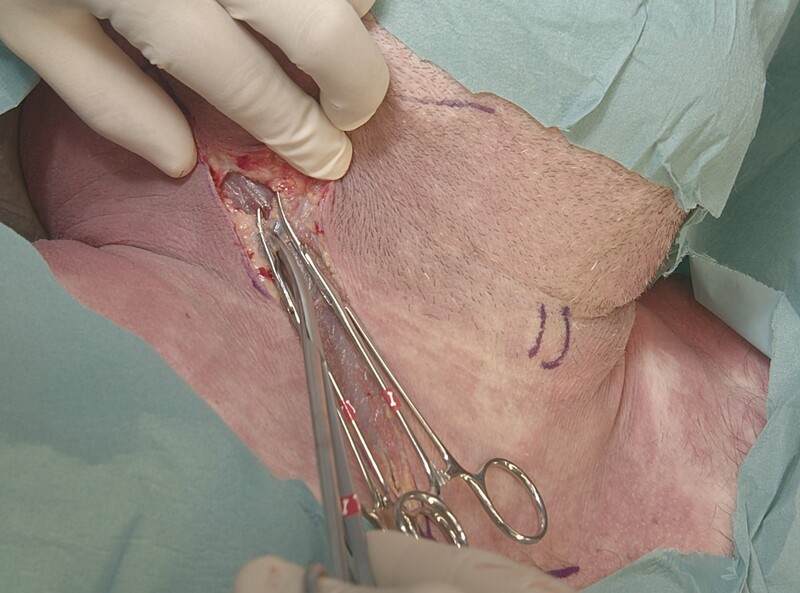
Landmarks and Incision Site
The sternocleidomastoid (SCM) muscle serves as the primary landmark, with the skin incision following its anterior border. If it is not palpable due to the injury or patient anatomy, the bony landmarks of its attachment points, the mastoid process and medial head of the clavicle, can be identified.
In a trauma situation, the incision is typically made full length from the mastoid process to the sternal notch level for proximal and distal vascular control, but it can be shortened based on injury location.
The angle of the mandible is marked for the transition between Zone 2 and Zone 3. The laryngeal prominence is the landmark for midline.
Skin Incision and Advancing to the Fascia
The skin incision is made with a scalpel or diathermy along the planned line to the subcutaneous fat level.
As the thin subcutaneous fat layer is divided, the platysma muscle becomes visible as the first organized muscular layer encountered.
The platysma fibers are divided along the length of the skin incision.
The deep cervical fascia, along with superficial veins, is seen underneath the platysma.A branch of the external jugular vein is ligated with sutures or electrocautery to maintain visibility.
With the platysma divided to the full incision length, the deep cervical fascia covering the sternocleidomastoid muscle becomes visible.
Log in or subscribe to access full content and see all the images.
Exposing the Sternocleidomastoid Anterior Edge
The aim is to expose the anterior surface of the sternocleidomastoid muscle and identify its medial border.
Controlled dissection with scissors is performed on the surface of the sternocleidomastoid muscle. The spinal accessory nerve penetrates the muscle in its upper third, so all dissection should happen on the surface of the muscle and not through it.
Once the anterior edge is clearly defined, retractors can be positioned to hold the superficial tissues aside, providing clear visualization of the muscle margin throughout the length of the incision.
Mobilizing and Retracting the Sternocleidomastoid
The aim is to retract the sternocleidomastoid laterally, providing exposure of the carotid sheath underneath.
Sharp dissection is used to free the sternocleidomastoid muscle along its medial edge.
The muscle edge is mobilized along the length of the incision. Superiorly, the spinal accessory nerve needs to be protected.
Perforating vessels entering the muscle should be coagulated or ligated before division.
Retractors are placed deeper until the sternocleidomastoid muscle can be fully retracted laterally. In a living patient, the carotid pulsation would guide the direction toward the carotid sheath.
Exposing the Carotid Sheath Proximally
The goal is to identify and expose the carotid sheath, which contains the major vascular structures of the neck.
The omohyoid muscle is identified in the caudal portion of the wound, running obliquely across the field.
The omohyoid muscle can be divided if proximal access to the carotid sheath is desired. This exposes the proximal internal jugular vein within the carotid sheath.
Opening the Carotid Sheath
The internal jugular vein (IJV) is exposed throughout the incision.
The carotid sheath is opened carefully, avoiding injury to the internal jugular vein.
The opening is continued cranially.
The carotid sheath is opened sufficiently when the internal jugular vein is visible throughout the incision.
Exposing the Internal Jugular Vein
The goal is to expose the internal jugular vein to be able to retract it aside to gain access to the common carotid artery.
The approach to the common carotid artery can be achieved either anterior or posterior to the IJV. In this case, both methods are shown and the vein is fully mobilized and looped for optimal exposure.
When dissecting around the neck veins, tissue traction should be gentle and sharp dissection is preferred over blunt spreading. Neck veins are fragile and tear easily. The repair is difficult after blunt stretch injury. Additionally, the vagus nerve runs within the same carotid sheath and must be carefully preserved during dissection.
The vein is now exposed and mobilized sufficiently to accommodate vessel loop placement and retraction.
Retracting the Internal Jugular Vein
The internal jugular vein can be retracted either anteriorly or posteriorly, providing access to the common carotid medial to it, without injuring the vagus nerve.
The method of retraction is a matter of preference; here, a vessel loop is used. The vessel must be adequately freed from surrounding tissues to allow safe passage of instruments without injuring the fragile vessel wall or adjacent carotid sheath structures.
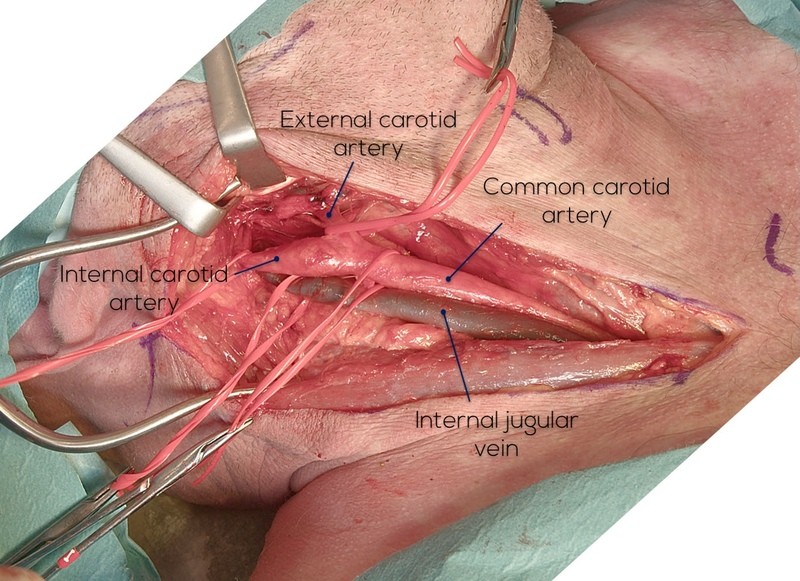
When the vein is retracted anteriorly, the common carotid artery becomes clearly visible and the retrojugular route has been accomplished.
The vagus nerve is identified posteriorly inside the carotid sheath.
Exposing and Controlling the Common Carotid Artery
For carotid artery injuries, achieving proximal control is essential before addressing the injury site. The approach should be aimed proximal to hematoma, to the uninjured part. If possible, distal control should also be obtained, as backflow can be extensive.
The approach should be made sharply to the arterial surface to visualize the vasa vasorum, and after that, the sheath is opened more extensively.
The fundamental principle when dissecting the carotid artery is to manipulate it as little as possible and never grasp it directly with instruments. Gentle technique is essential to avoid intimal damage, dissection, or dislodging atherosclerotic plaque.
The common carotid artery has no branches before the bifurcation level, making exposure of this segment relatively straightforward, though careful technique with the instruments remains essential.
The vagus nerve is in close proximity and is kept protected at all times when working in the carotid sheath.
The artery is carefully encircled proximal to the injury area, and a vessel loop is passed around it.
A single loop provides gentle vessel control for mobilization and can be easily moved proximally as exposure is extended superiorly.
Here, a double loop is done, offering more secure control and allowing temporary occlusion without clamps when working on the injured area.
If occlusion is performed, the patient should be heparinized to minimize the risk of embolic events affecting the central nervous system.
Exposing the Carotid Bifurcation
The goal is to expose the common carotid cranially to reach the level of the bifurcation. The typical level is at the superior border of the thyroid cartilage or C3–C4 vertebral level.
A good landmark for locating the bifurcation intraoperatively is to identify the facial vein branching from the internal jugular vein, which is typically located at the same level.
The internal jugular vein is exposed cranially until the facial vein is identified anteriorly.
As the vein is retracted aside, the caliber of the common carotid begins to widen, marking that the bifurcation level has been reached.
Identifying the External and Internal Carotid Arteries
The aim is to distinguish between the internal and external carotid arteries. This is critical for trauma management, as the internal carotid requires repair while the external carotid can be ligated if necessary.
The external carotid artery can be identified by the presence of branches, while the internal carotid normally has no extracranial branches in the neck.
The first branch is visible, the superior thyroid artery, confirming that the more medial vessel is the external carotid artery.
The confirmed internal carotid artery shows here the characteristic thicker proximal enlargement of the carotid sinus area. This is an extremely delicate area requiring utmost care during dissection. Stimulation of the carotid sinus may provoke vagal responses like bradycardia and hypotension.
Isolating and Controlling Carotid Arteries
Both carotid arteries are exposed further cranially to allow vessel loop control. The hypoglossal nerve should be protected.
The external carotid artery is gently secured with careful vessel loop placement.
After the loop has been placed, the fan-like appearance of the external carotid artery can be appreciated, with its multiple branches visible here. The main trunk has now been secured with the loop.
Due to limited space for controlling the internal carotid artery while protecting the hypoglossal nerve, the facial vein is ligated at this point to improve exposure and demonstrate the antejugular approach to the carotid arteries.
The vein is clamped proximally and distally, divided, and both ends are ligated.
A transfixing ligature is used to secure the stump at the internal jugular vein side.With the facial vein now ligated, better exposure of the bifurcation level is in this case achieved through the antejugular route.
This also reveals the hypoglossal nerve running close to the bifurcation.
It requires identification and careful preservation; here, a vessel loop is placed around it for a gentle hold before encircling the internal carotid artery.
The hypoglossal nerve can sometimes be located using the ansa cervicalis as a landmark, since its superior root travels with the hypoglossal nerve. The ansa cervicalis is a nerve loop innervating most strap muscles and runs along the carotid sheath. While ansa cervicalis preservation is preferred, it may be sacrificed for exposure, but the hypoglossal nerve must always be preserved.
With the hypoglossal nerve protected, the internal carotid artery can now be carefully encircled.
Vascular control of both the external and internal carotid arteries has been achieved, with the hypoglossal nerve protected.
Distal Exposure of the Internal Carotid Artery
The aim is to expose the internal carotid artery as far cranially as possible to demonstrate the maximal extent achievable through this approach. This is particularly relevant for high neck injuries near the skull base, where surgical access becomes increasingly challenging. While endovascular techniques are typically preferred for such injuries, understanding the anatomical limits of open surgical exposure remains essential.
Additional exposure can be obtained using several methods. Part of the salivary gland tissue has been mobilized here to demonstrate the cranial anatomy.
If the parotid/submandibular gland is injured during the original trauma, the principle is to avoid excessive manipulation and allow ENT specialists to manage the injury. A drain should be placed to prevent fluid accumulation.The posterior belly of the digastric muscle runs from the mastoid notch to the hyoid bone and can be divided to gain better access. If the muscle is divided, it should be done at the avascular tendinous part and the ends marked with sutures for repair upon closure.
The glossopharyngeal nerve is seen here coursing deep to the digastric muscle. It represents a critical structure in this higher region and must be protected when approaching the skull base.
At this level, the mandible creates significant anatomical obstruction. While vascular structures might remain visible, operative access becomes extremely limited in a trauma setting. Some additional space can be generated by subluxating the mandible anteriorly.
Recap of the exposed vascular structures in the lateral neck:
Proximally, this approach provides exposure down to the manubrial edge. The common carotid artery origin, branching from the brachiocephalic trunk alongside the subclavian artery, can be visualized through the lateral neck approach, but access to gain control of these vessels is typically achieved through endovascular methods or through sternotomy/supraclavicular incision.
Access to the Medial Structures
The lateral approach can be used to access the medial structures, exposing the trachea and esophagus for evaluation and treatment of potential injuries.
The thyroid gland is identified by the vasculature on its surface. It often obstructs access to the medial structures with the lateral approach, and typically requires mobilizing or, in some cases, resection.
Above the thyroid, access to the pharynx and larynx can be obtained if needed.
Posterior to the larynx/pharynx, the cervical spine is also accessible.
Anterior to the thyroid are the strap muscles. Access beneath these muscles is usually possible by identifying the appropriate tissue plane and proceeding in an avascular layer.
If the thyroid requires mobilization, the inferior pole vessels can be divided if needed for more exposure. Importantly, when dissecting posterior to the thyroid, the recurrent laryngeal nerve must be identified and protected from injury.
On the right side, the nerve runs more medially than on the left side.The tracheal cartilage rings can be palpated and they become visible once the thyroid is mobilized superiorly.
The recurrent laryngeal nerve runs in the groove alongside the trachea and must be carefully preserved. Damaging it leads to vocal cord paralysis on the affected side and can affect swallowing.The superior part of the esophagus can be approached bluntly posterior to the trachea, medial to the common carotid. If the patient has a nasogastric tube, identification is easier. The esophagus can be encircled and repaired through a lateral neck incision, but especially with complex injuries, bilateral exposure and/or a collar incision may be required.
Hemostasis and Closure
For extensive dissections and complex injuries, closed suction drains are placed to reduce postoperative swelling and provide early warning of potential postoperative bleeding.
Divided digastric or omohyoid muscles should be reconstructed, while the carotid sheath and sternocleidomastoid muscle require no suturing.
The actual wound is closed in two layers, starting with the platysma, which is closed using running 2-0 or 3-0 absorbable sutures in a single layer.
The skin can be closed with either intracutaneous sutures or running monofilament sutures. Staples are avoided because they are difficult to remove quickly if emergency re-exploration is needed.
To access the full video and additional content on this subject, log in or subscribe
Piftalls and Complications
Pitfalls
Not Securing the Airway Early
The airway should be secured early on. Prolonging the intubation to a “can’t ventilate, can’t intubate” scenario is a recipe for disaster. In such a case, a surgical airway might also prove challenging, and even in the event of technical success, it may unleash the previously contained bleeding.
IV Line Placed at the Side of Injury
The IV line should always be placed on the contralateral side of the injury. A Zone 1 injury may well mean a subclavian vein injury, and if the IV line is in the arm on the side of the injury, the infusions will have no access to circulation.
Operating Without Adequate Experience or Preparation
A successful trauma operation in the neck requires both skill and quick thinking. Operating on the neck is always a judgement call, and both general understanding of anatomy and surgical landmarks as well as manual dexterity are needed to deal with the neck. Ideally, knowledge of anatomy and feel for soft tissue handling should be acquired through elective surgery, whether it is vascular or glandular surgery. Furthermore, situational awareness of the whole operation and solid leadership are required for a successful trauma operation to the neck.
Wrong Incision Site
The placement of the skin incision is not self-evident if anatomy is distorted by hematoma or balloon tamponade. It is wise to choose virgin territory as a starting point, approaching the injury only after key structures are identified. The sternal notch is always palpable, as is the mastoid process.
Exploring Within the Hematoma
Direct dissection into the hematoma should not be performed. Instead, dissection should be started in normal, uninjured tissue away from the bleeding area, then the injury should be approached once key anatomical structures have been identified. If the dissection becomes difficult and tissue planes are unclear, re-orientation is needed.
Inadequate Hemostasis During Closure
Hemostasis should be ensured before closure, as even minor bleeding can accumulate in the confined cervical space and compromise the airway postoperatively.
Complications
Postoperative Re-bleeding
Postoperative re-bleeding can occur from hours after surgery to 2 weeks postoperative. Most bleeds present within 24 hours, justifying this minimum surveillance period. Significant neck swelling postoperatively warrants re-operation. In severe acute cases, the airway is secured by opening the wound at bedside before formal re-operation.
Delayed bleeds are equally dangerous as acute ones. The usual culprit is arterial recanalization due to failed clips or sutures, or unrecognized arterial injury from the primary trauma. All patients must be informed about potential late bleeding to ensure early recognition and intervention.
Reperfusion Injury
Prolonged clamping or compression (>1 hour) of the carotid arteries followed by restoration of flow can result in cerebral reperfusion injury. The ischemic brain tissue becomes vulnerable to oxygen free radical damage when circulation is restored, potentially causing cerebral edema, hemorrhagic transformation, and paradoxical neurological deterioration despite successful vascular repair.
Air Embolism
Large venous injuries, particularly to the internal jugular vein, can allow air entry into the venous system if the patient is in reverse Trendelenburg position. This can result in cardiovascular collapse and requires immediate recognition with patient positioning, wound flooding, and supportive measures.
Iatrogenic Nerve Injury
Operating on a traumatized neck is not a safe endeavor, so iatrogenic injuries may occur. The treatment of nerve injuries, for example recurrent laryngeal nerve injury, is mainly symptomatic but requires a multidisciplinary approach, including ENT, nutrition, and speech therapy, for optimal outcome.
Aftercare
General Guidelines
The aftercare protocols may vary between units.
Aftercare depends on the specific injury.
The wound itself commonly heals well; typically, no immobilization or prolonged antibiotic therapy is needed. Drains can usually be removed on the first postoperative day.
Patients are extubated early and laryngeal function is assessed. Any voice or swallowing abnormalities require ENT consultation.
Anticoagulation management is planned with vascular surgery. Arterial repairs typically receive antiplatelet therapy until intimal healing is complete.
FAQ
What is the goal of the lateral neck approach for penetrating neck trauma?
The goal is to expose critical vascular structures of the neck for diagnosis and treatment.
Which major vascular structures can be evaluated through this approach?
The approach provides access to the common carotid artery, internal and external carotid arteries, and internal jugular vein.
Which neural structures must be preserved during the approach?
Critical neural structures include the vagus nerve within the carotid sheath, the hypoglossal nerve near the carotid bifurcation, the glossopharyngeal nerve in the upper neck, and the recurrent laryngeal nerve running between the trachea and esophagus.
Why is intravenous access placed on the side opposite the injury?
The IV line should be placed contralateral to the injury because a Zone 1 injury may involve the subclavian vein, and an IV line on the injured side may not provide access to the circulation.
Why should direct dissection into the hematoma be avoided?
Direct dissection into the hematoma should not be performed. Dissection should start in normal, uninjured tissue away from the bleeding area, and the injury should be approached only after key anatomical structures have been identified.
What postoperative finding may require re-operation?
Significant postoperative neck swelling warrants re-operation. In severe acute cases, the airway is secured by opening the wound at bedside before formal re-operation.
When can drains usually be removed?
Drains can usually be removed on the first postoperative day.
What should be done if voice or swallowing abnormalities occur after surgery?
Any voice or swallowing abnormalities require ENT consultation.
To access the full video and additional content on this subject, log in or subscribe