How to perform a suprapubic catheter placement
Source
To access the full video and additional content on this subject, log in or subscribe
Summary
Focus: Creating a urinary pathway from the bladder in patients with urinary retention when urethral catheterization is not an option.
Key elements: Adequate bladder fullness, correct midline insertion site, appropriate trocar angle, and avoiding overly deep insertion are central to safe catheter placement.
Indications and Clinical Context
General
Medical expert: Petrus Järvinen, urologist
Name of procedure: Suprapubic catheterization, suprapubic cystostomy, percutaneous cystostomy
Goal of Procedure
Creating a urinary pathway from the bladder in patients with urinary retention if urethral catheterization is not an option.
Problem
Urinary retention
Diagnosis
Urinary retention (ICD-10: R33)
Short Pathophysiological Description
Urinary retention can be caused by any process obstructing the urethra. Common causes include benign prostatic hyperplasia, urethral stricture, prostate cancer, and urethral injuries, such as a false passage created during catheterization attempts. Tumors located at the bladder neck, bladder stones, and certain medications, such as anticholinergics, antihistamines, tricyclic antidepressants, and opioids, can also lead to urinary retention. Neurological causes, such as diabetic neuropathy, spinal cord injury, or cerebral events, can also cause urinary retention.
Key Anatomical Structures
Bladder
Pubic symphysis
Midline
Peritoneum
Bowel
Prostate
Uterus
Iliac vessels
Step-by-Step Technique
Patient Positioning and Preparation
The patient is supine.
The lower abdomen is exposed, draped, and prepped in a sterile manner.
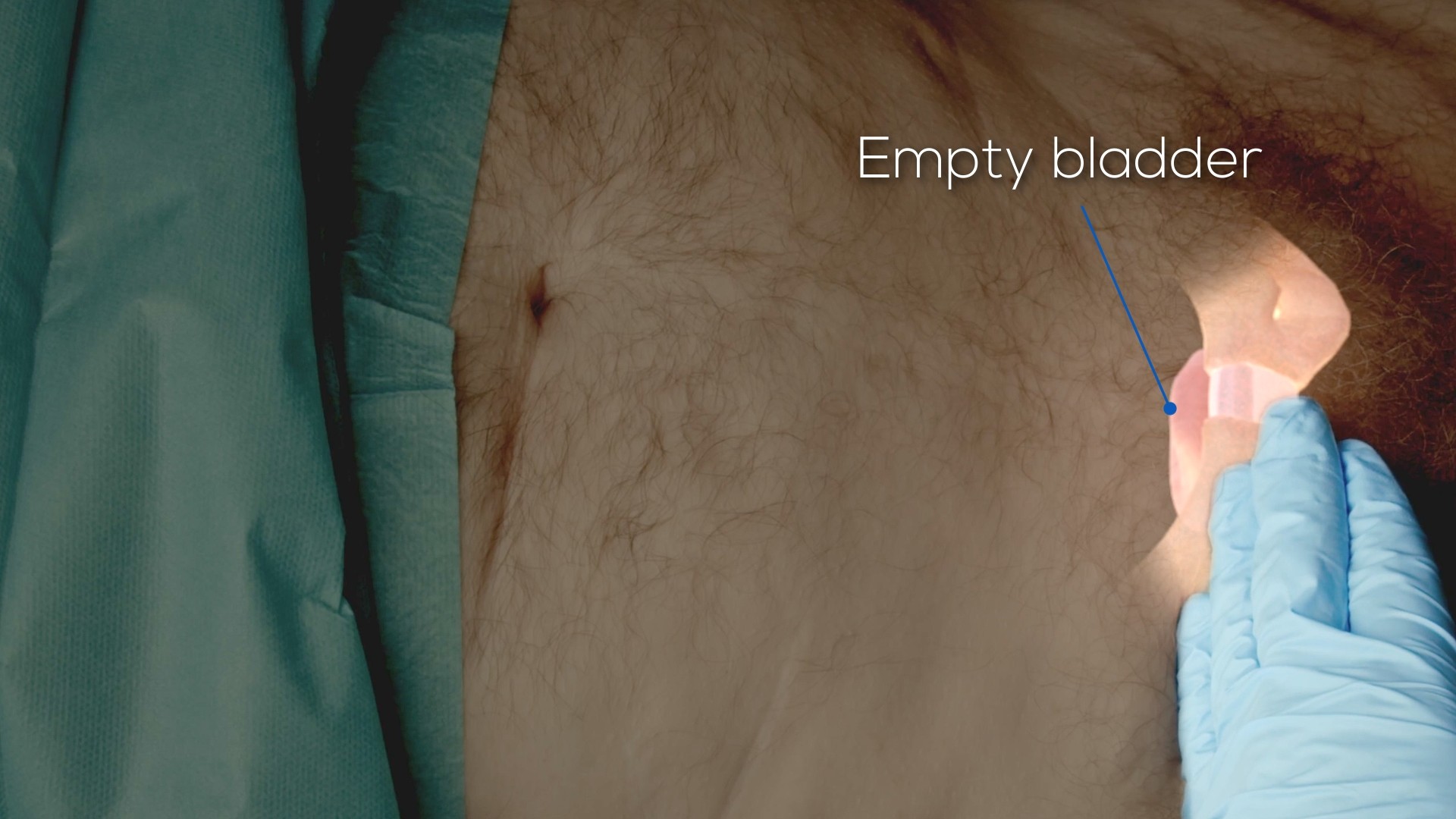
The bladder should be full, up to 300–400 ml. If the bladder is empty, it is situated behind the pubic symphysis, and inserting a catheter poses a significant risk of peritoneum and bowel perforation.
Ultrasound can be used to verify bladder fullness.
Log in or subscribe to access full content and see all the images.
Landmarks and Insertion Site
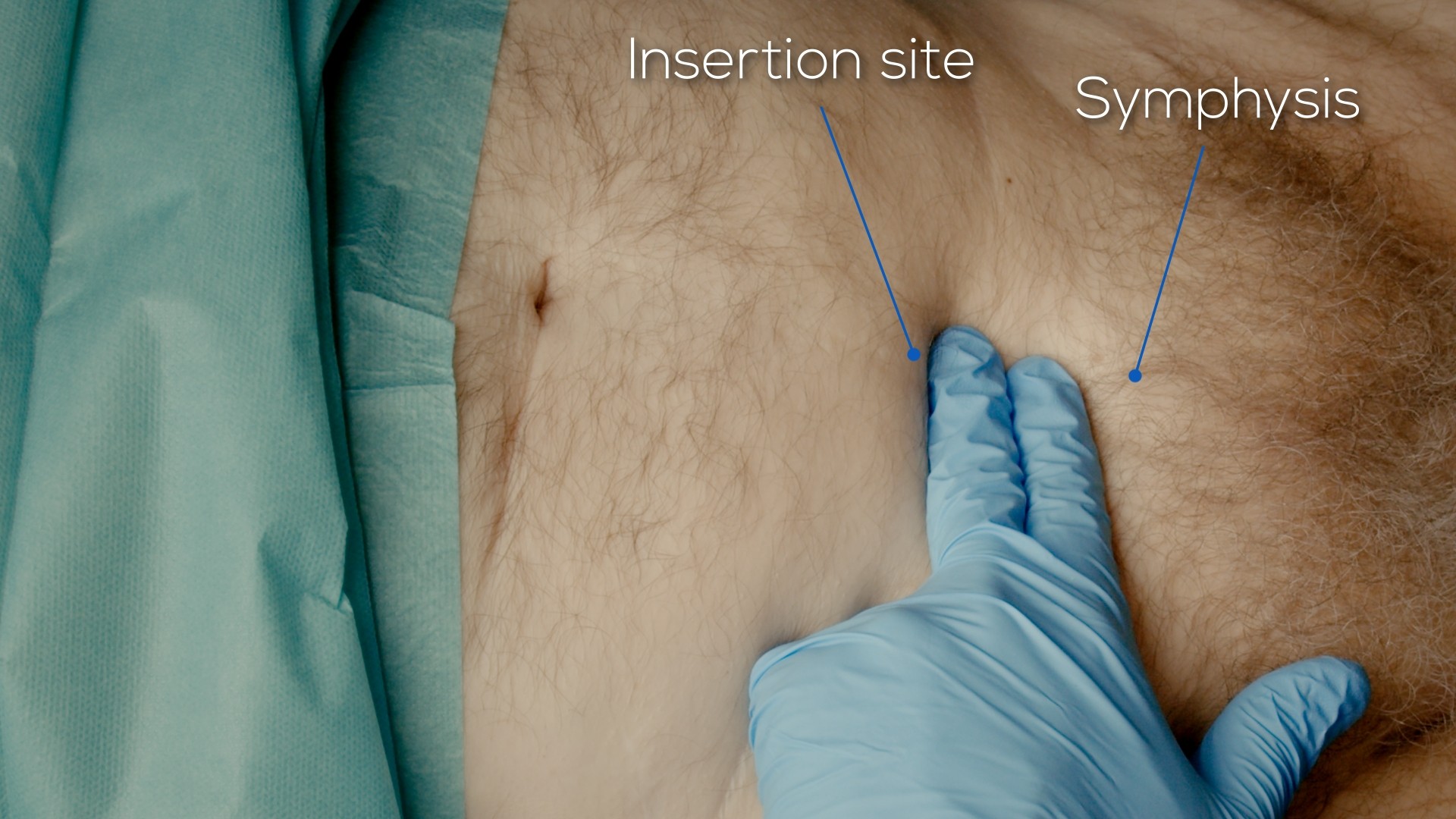
The landmarks for the insertion site are the midline, guided by the navel, and the pubic symphysis.
A safe insertion site, provided that the bladder is full, is 2 finger-widths above the pubic symphysis in the midline. A higher insertion site or under-filled bladder risks bowel injury and peritonitis. Inserting lower might potentially damage the urethra or the prostate. Deviation from the midline can, in the worst-case scenario, risk the iliac vessels.
Log in or subscribe to access full content and see all the images.
Local Anesthesia
For example, lidocaine with a long needle can be used to anesthetize the procedure area according to the landmarks.
The skin area of the insertion site should be anesthetized first.
Deeper tissues are anesthetized by positioning the syringe plunger upwards, simulating the path to the bladder while simultaneously gradually injecting the anesthetic.
The bladder wall can typically be felt as increased resistance. The needle can be passed into the bladder. Aspiration of urine confirms the correct location.
Inserting the Catheter
The scalpel from the catheter set can be used to make the skin incision according to the landmarks.
The incision is done transversely, 1–2 cm in length, incising all the skin layers.
The catheter is guided into the bladder through the deeper tissue layers with the help of a trocar. If the catheter is placed inside the trocar when inserting, it should be kept away from the sharp tip of the trocar to avoid damaging it.
The trocar should be positioned with its end pointing upwards. An incorrect angle of insertion might lead to injury.
The trocar can be gently pressed with slight drilling motion through the bladder wall.
When the resistance is no longer felt, the trocar tip is inside the bladder. The index finger can be used as a stopper to avoid advancing too deep and possibly injuring the rectum or the uterus.
When the trocar tip is in the bladder, the catheter can be inserted deeper into the bladder.
The trocar is then pulled out and split while keeping the catheter in the bladder.
The balloon is inflated with an adequate amount of fluid stated in the catheter, typically 10 ml.
The catheter is gently pulled to confirm that the balloon is fully inflated.
One suture can be applied to seal the skin incision if there is bleeding. Wound tape can be applied to the base of the catheter.
To access the full video and additional content on this subject, log in or subscribe
Piftalls and Complications
Pitfalls
Insufficient Bladder Fullness
When the bladder is full, it rises above the pubic symphysis, providing a clearer area for catheter insertion. A fuller bladder also pushes the intestines upward, decreasing the risk of injuring the bowel. If the bladder is not full, it remains lower, increasing the chance of bowel complication.
Wrong Insertion Site
A trocar placed too cranially may lead to bowel injury. Conversely, a trocar placed too caudally might harm the prostate or urethra. Straying from the midline can put the iliac vessels in danger. Typically, an insertion site in the midline and two finger-widths above the pubic symphysis is considered safe, provided that the bladder is adequately full.
Incorrect Angle of Insertion
The end of the trocar should face upwards during insertion.
An incorrect angle might lead to damage to the surrounding tissues.
Inserting the Trocar Too Deep
Inserting the catheter too deep can pierce the posterior wall of the bladder and, in the worst case, cause rectum injury or, in females, injure the uterus. The trocar should not be inserted into an empty bladder, and the pushing of the trocar should be stopped once it has passed through the anterior wall of the bladder. The index finger can be used as a stopper.
Complications
Bowel Injury
If the trocar penetrates the peritoneal cavity due to an underfilled bladder or an incorrect insertion site or angle, it poses a risk of bowel injury and peritonitis. The most reliable method to check the level of bladder fullness is through ultrasound. The trocar should not be inserted too deeply, and the insertion should cease once it has penetrated the anterior wall of the bladder. If there is suspicion of bowel injury during catheter placement, a lower abdominal CT scan should be performed.
Injury to the Prostate or the Uterus
A trocar inserted at an incorrect angle or level could damage the prostate, potentially leading to bleeding. Hematuria resulting from prostate bleeding is usually treated with an irrigation catheter. Sometimes, surgical hematoma evacuation is needed. In females, a trocar inserted too deeply could affect the uterus. The bladder should be full at procedure start. Insertion should stop once the bladder's anterior wall is penetrated.
Vascular Injury
A puncture deviating from the midline, directed too laterally, can cause vascular injuries that, at worst, can threaten hemodynamics.
Aftercare
General Guidelines
The catheter is connected to a collection bag or, in some cases, alternatively capped.
Slightly reddish urine is not dangerous. If the urine is significantly bloody, a urethral catheter can be placed and the bladder irrigated until the bleeding stops.
The patient should not be in much pain after catheter placement. If the patient is in pain, the possibility of complications should be kept in mind and CT imaging considered.
FAQ
What bladder volume is recommended before suprapubic catheter placement?
The bladder should be full, up to 300–400 ml. Ultrasound can be used to verify bladder fullness.
Where is the safe insertion site?
Provided that the bladder is full, a safe insertion site is in the midline, 2 finger-widths above the pubic symphysis.
What confirms the correct location during local anesthesia?
Aspiration of urine confirms the correct location.
What should be considered if the patient is in pain after catheter placement?
The patient should not be in much pain after catheter placement. If the patient is in pain, the possibility of complications should be kept in mind and CT imaging considered.
To access the full video and additional content on this subject, log in or subscribe