How to perform a traumatic finger amputation revision
Source
Surgeon:
Matti Mustaniemi (hand surgeon)
To access the full video and additional content on this subject, log in or subscribe
Summary
Focus: Revision of traumatic finger amputation to achieve a neat, painless, and maximally functional finger.
Key elements: Evaluation, hemostasis, anesthesia, wound revision, bone shortening, nerve resection, wound closure, pitfalls, complications, and aftercare.
Indications and Clinical Context
General
Medical expert: Matti Mustaniemi (hand surgeon), Anna Ikonen (orthopedic surgeon)
Name of Procedure: Revision of traumatic finger amputation
Goal of Operation
To achieve a neat, painless, and maximally functional finger.
Problem
Traumatic amputation or unsatisfactory stump healing.
Diagnosis
Traumatic transphalangeal amputation of finger (ICD-10: S68.6)
Short Pathophysiological Description
Revision may be needed after a partial or total traumatic finger amputation. In trauma-related finger amputations, once any possibility of replantation has been excluded, it is important to ensure the injury heals swiftly and without complications. Typical causes of trauma are the use of power tools and machines. The extent to which the finger is fractured or crushed varies. The choice of treatment is determined by the level and direction of the injury. In avulsion injuries, there are several broken surfaces, so the level of the final amputation is determined by the sensory and motor functions as well as the amount of residual intact skin. In nail injuries, total removal should be considered if the nail cannot be expected to heal properly.
Key Anatomical Structures
Phalanges and joints
Flexor tendons
Flexor digitorum superficialis (FDS)
Flexor digitorum profundus (FDP)
Neurovascular bundles of the finger
Nail, nail matrix, and nail bed
Step-by-Step Technique
Evaluation, Hemostasis, and Anesthesia
A plain radiograph with the affected finger still in prehospital bandages should be considered before other examinations.
Local anesthetic should be administered for pain relief as early as possible, once the neurological evaluations have been made.
Cleaning the wounds with saline solution is not recommended until after anesthesia.
A tourniquet, such as a rubber band, should be applied if possible, even before anesthesia if necessary.
Wound Revision
Debride and trim ragged wound edges. Remove dirt, foreign bodies, and non-vital tissue.
Make additional incisions to both ulnar and radial sides of the finger to gain a better field of exposure and to assist with closure.
Intact, functional tendons should be preserved. Those beyond repair should be incised as proximally as possible.
If it does not seem like a healthy nail is achievable, the entire nail matrix and the nail bed should be excised.
Log in or subscribe to access full content and see all the images.
Bone Shortening
Shorten the bone as necessary to allow unrestricted skin closure. Make sure to spare the base of the digit and to not crush the bone when using a small rongeur. To achieve optimal results, tiny precise bites of the bone are preferred, and cutting the bone either by twisting or using a larger rongeur should be avoided. Unnecessary force may cause a fracture in the diaphysis of the bone or the base of the digit.
Sharp edges should be smoothed and any bone chips removed. You can use your own gloved finger to feel for sharp edges of bone that need to be resected.
If the amputation is at joint level, joint cartilage should be removed. This will also help in making the stump feel less bulky.

Log in or subscribe to access full content and see all the images.
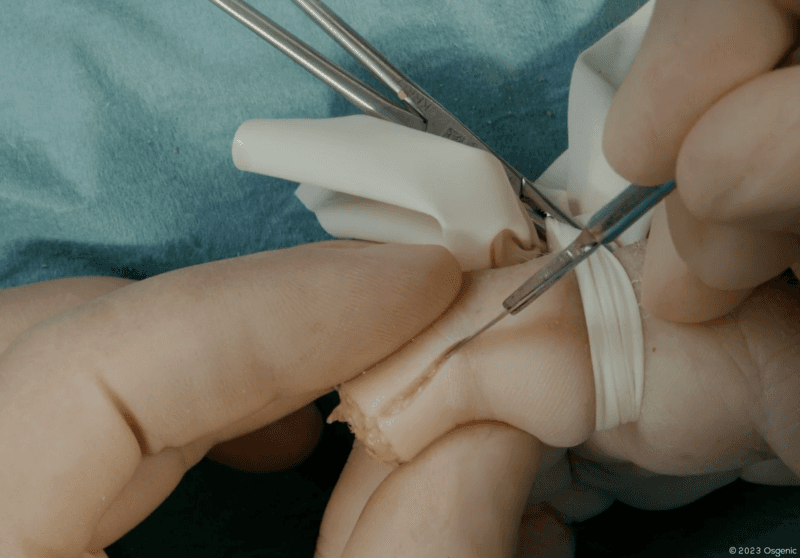
Nerve Resection
The affected nerves should be severed as far away from the wound as possible. This will prevent the nerves from adhering to the distal edges of the stump and thus causing hypersensitivity or a painful neuroma. After excision, the nerve will also retract, but it is important to cut the nerves proximally rather than distally.
Distally, much of the dorsal sensory function is provided by a dorsal nerve branch that stems from the volar main branch. If encountered, this nerve branch should be resected as well.
Make sure to check you’re not confusing the nerve with vascular structures. The nerves have no lumen and are a light yellow color.
Wound Closure
If the digital artery or smaller vessels are seen, they can be sealed with precise use of the diathermy to avoid a hematoma that might cause a complication for the healing of the stump. Excessive use of the diathermy should be avoided so as not to cause damage to the tissue.
Neat skin closure without tension is important for primary healing. For example, a 4-0 suture is easy to remove and difficult to overtighten. Starting at the center of the wound is an easy way to make sure there isn’t too much tension and that the edges of the wound align symmetrically. As the wound closure progresses, be critical in assessing the result and remove unnecessary sutures in order to achieve optimal tension.
Do not cut the sutures too short, as the sharp ends or knots may cause pain. In an ER setting, it sometimes helps to leave the ends of a single suture significantly longer and then use this suture as a tool to help place the finger in different positions.
Finally, place the dressings before releasing the tourniquet because some bleeding is always to be expected.
To access the full video and additional content on this subject, log in or subscribe
Piftalls and Complications
Pitfalls
Too Tight Skin Closure
Skin tightness compromises good wound healing. When the skin closure is too tight, after finally healing, the stump tip may be very hard and tender.
Digital Nerve End Left Too Long
If digital nerve is left too long, and it attaches to the wound during healing, it will cause hypersensitivity of the skin or painful neuroma formation. Nerves should be sufficiently shortened proximally, away from the wound site and sutures.
Careless Cartilage Removal
When the amputation level is at the joint, the cartilage should be carefully removed. Any remaining cartilage may cause exudation and wound problems.
Not Removing the Nail Bed When Necessary
If good nail growth cannot be achieved, the entire matrix and nail bed should be removed. Otherwise, small nail spikes may grow. Meticulous removal is tedious work but will prevent further operations.
Too Aggressive Bone Shortening
Overly aggressive shortening of the bone end may cause injuries to proximal structures. Use the rongeur with care and precision. Do not exert extra force or use a twisting motion, which might splinter the diaphysis or crush the base of the phalanx.
Complications
Perioperative Fractures
Perioperative fractures may be caused by overly aggressive shortening of the bone. Careful and precise use of the rongeur and avoiding extra force or using a twisting motion may prevent splintering the diaphysis or crushing the base of the phalanx.
Infection
Osteitis is the most significant infectious complication. Both the trauma itself and poor cleaning of the injury site are predisposing factors. Use a sufficient amount of saline solution for painstaking debridement of foreign matter in the wound. Depending on the contamination level, a prophylactic antibiotic should be administered and tetanus booster considered.
Postoperative Pain/Tenderness
If a severed digital nerve adheres to the edges of the wound, the scar of the amputation stump may become very tender. Ensure nerves are sufficiently shortened proximally, away from the wound site and sutures.
Aftercare
General Guidelines
Ensure good pain management.
The first change of bandage dressing should occur 3–5 days after the operation.
From then on, daily showering is recommended and a light dressing should be applied.The sutures should remain for at least two weeks. If the wound is still swollen at two weeks, you can also remove every other suture and keep monitoring the wound until the removal of all sutures seems safe.
Use of the affected finger is encouraged as soon as possible, pain and wound permitting.
FAQ
What is the goal of revision of traumatic finger amputation?
The goal is to achieve a neat, painless, and maximally functional finger.
When may revision be needed after traumatic finger amputation?
Revision may be needed after a partial or total traumatic finger amputation, or when stump healing is unsatisfactory.
Why should nerves be shortened proximally?
Nerves should be sufficiently shortened proximally, away from the wound site and sutures, to prevent hypersensitivity or painful neuroma formation.
When should the nail matrix and nail bed be removed?
If good nail growth cannot be achieved, the entire matrix and nail bed should be removed to prevent small nail spikes and further operations.
To access the full video and additional content on this subject, log in or subscribe