How to perform a urethral catheter placement
Source
To access the full video and additional content on this subject, log in or subscribe
Summary
Focus: Urethral catheterization to facilitate bladder drainage or access by inserting a catheter through the urethra into the bladder.
Key elements: Patient preparation, catheter insertion, balloon inflation, aftercare, pitfalls, and complications.
Indications and Clinical Context
General
Medical expert: Petrus Järvinen (urologist)
Names of Procedure: urethral catheterization, urinary catheter placement, Foley catheter placement, bladder catheterization
Goal of Operation
To facilitate bladder drainage or access by inserting a catheter through the urethra into the bladder.
Problem
Typically: retention, hematuria or preoperative preparation
Diagnosis
Urinary retention (ICD-10: R33)
Hematuria (ICD-10: R31)
Short Pathophysiological Description
Urethral catheterization provides a direct pathway for urine to exit the body when normal urination is not possible. By bypassing obstructions or compensating for lack of bladder control, it allows for the immediate relief of urinary retention. This not only alleviates discomfort but also prevents potential kidney damage from backflow of urine. In cases of hematuria, catheterization flushes out blood clots that may be blocking the urinary tract.
Key Anatomical Structures
Urethra
Bladder
Prostate
Step-by-Step Technique
Patient Positioning and Preparation
The patient is supine with legs slightly apart.
The foreskin, if present, is retracted and the glans, the sulcus behind it, and the urethral meatus are swabbed.
The urethra is lubricated with a local anesthetic gel, such as lidocaine gel, which also aids in dilating the urethral passage and providing some degree of anesthesia. The lubricant is applied generously, for example, 2 tubes directly into the urethra.
Inserting the Catheter
The standard urinary catheter is a 2-way silicone Foley in size 14–16 Fr for adult males. Upsizing is recommended in conditions like hematuria with clots. A 3-way catheter is selected when irrigation is needed. A Coude curved tip is considered if the insertion is difficult.
To straighten the urethra's natural curve before catheter insertion, the penis should be oriented upwards.
The catheter is inserted into the urethra with care, ensuring it slides forward smoothly.
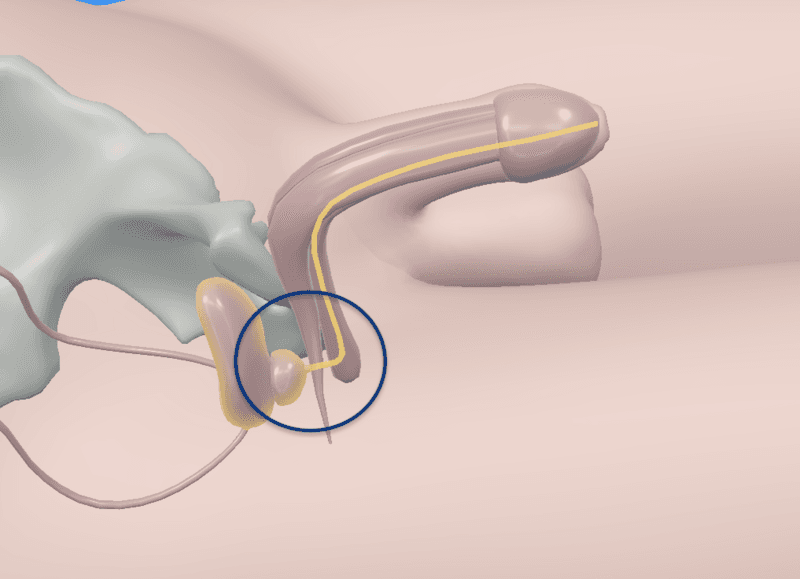
Some resistance can be felt around the prostate area. The urethra also naturally curves in a more ventral direction before reaching the prostate level.
If insertion becomes difficult at this point, gentle pressure applied to the perineum can assist in advancing the catheter.When the catheter has reached the bladder, the outflow of urine will confirm correct placement.
The catheter should be inserted fully to ensure that the balloon is positioned within the bladder and not at the level of the urethra.
Log in or subscribe to access full content and see all the images.
Inflating the Balloon
In a dual-lumen catheter, one channel facilitates the outflow of urine, while the other is used to inflate the balloon.
The balloon is inflated with sterile water, typically 10 ml, or as indicated on the catheter itself. Exceeding this volume should be avoided to prevent the balloon from bursting.
Resistance felt during inflation may indicate incorrect balloon placement, potentially causing urethral damage.Once the balloon is inflated, the catheter can be gently pulled back to ensure the balloon is fully inflated and correctly positioned within the bladder.
The foreskin, if present, should be returned to its original position to prevent the development of paraphimosis.

Log in or subscribe to access full content and see all the images.
To access the full video and additional content on this subject, log in or subscribe
Piftalls and Complications
Pitfalls
Insufficient Lubrication
Insufficient lubrication can make catheter insertion difficult, potentially leading to an unsuccessful procedure. Additionally, it can increase patient discomfort and risk of urethral trauma.
Forceful Insertion
The catheter should never be inserted forcefully, as this can result in creation of a false passage or urethral perforation. If resistance is encountered and cannot be resolved with gentle manipulation or additional lubrication, an evaluation should be done to identify the cause, which could include a urethral stricture, prostate obstruction, bladder stones, a foreign body, or a tumor.
Premature Balloon Inflation
If the balloon is inflated prematurely, while still within the urethra, typically in the prostate, it can cause significant trauma and pain. To avoid this, the catheter should be fully inserted first, then inflated, and only then pulled back to check the hold.
Long-Term Use
Prolonged catheterization increases the risk of urinary tract infections, urethral damage, erosion, and bladder stones. Catheters should be used for the shortest time possible and regular assessments should be conducted to determine if continued use is necessary.
Complications
Urethral Trauma
Potential damage to the urethral tissue may occur during catheter placement leading to urethral strictures, hematuria, false passages, and increased risk of infections. This can be mitigated by ensuring the catheter is inserted and removed gently, and by using sufficient lubrication. If clear resistance is met, the procedure should be stopped and reassessed.
False Passage
False passage refers to an artificial channel creation into the periurethral tissues. The risk increases with prior urethral alterations due to instrumentation, trauma, radiation therapy, or infections. To prevent this, a correct catheterization technique, involving appropriate catheter choice, sufficient lubrication, and gentle insertion should be applied.
Urethral Erosion
Urethral erosion may occur due to prolonged catheter use. This risk can be minimized by ensuring the catheter is not left in place longer than necessary and by regular monitoring for signs of urethral injury.
Urinary Tract Infections
Urinary catheterization can lead to urinary tract infections, especially when the catheter remains in place for a long time. The insertion can introduce bacteria into the urinary tract, and damage to the urethra can increase UTI risk. To minimize the risk, a proper insertion technique, aseptic protocol, and the removal of the catheter as soon as possible are essential.
Aftercare
General Guidelines
A closed sterile drainage system is maintained to prevent contamination and infection.
The catheter tube is secured to prevent movement and urethral traction. The catheter and collecting tube are kept free from kinking.
The duration a urethral catheter is left in place can vary based on individual circumstances and medical needs. However, it is important to keep the catheterization period as short as possible to minimize risks of urinary tract infections and damage to the urethra, for example erosion.
FAQ
What confirms correct catheter placement?
When the catheter has reached the bladder, the outflow of urine will confirm correct placement.
What is the typical balloon inflation volume?
The balloon is inflated with sterile water, typically 10 ml, or as indicated on the catheter itself.
Why should the catheter be inserted fully before balloon inflation?
The catheter should be inserted fully to ensure that the balloon is positioned within the bladder and not at the level of the urethra. Premature balloon inflation while still within the urethra, typically in the prostate, can cause significant trauma and pain.
Why should the foreskin be returned to its original position?
The foreskin, if present, should be returned to its original position to prevent the development of paraphimosis.
To access the full video and additional content on this subject, log in or subscribe